What Is Uterine (Endometrial) Cancer?
Uterine cancer is a cancer that begins in the lining of the uterus (called the endometrium). It is the most common gynaecological cancer in many parts of the world and most often affects women after menopause.
There are two main types:
- Endometrial cancer (most common): Starts in the lining of the uterus
- Uterine sarcoma (rare): Develops in the muscles or other tissues of the uterus
Global Statistics
- Uterine cancer is ranked as the second most common gynaecological malignancy worldwide, with 420,242 new cases and 97,704 deaths reported in 2022. It is the most common gynaecological cancer in many parts of the world. In high-income countries, it accounts for 50% or more of all gynaecological cancer cases.
- Mortality: While survival rates are generally high for early-stage uterine cancer, the disease can be deadly if diagnosed at a later stage.
- Trends: The incidence of uterine cancer is rising, particularly among women aged 60 and older. This increase is attributed to factors such as obesity, diabetes, and the use of hormone replacement therapy.
Who Is at Risk?
- Postmenopausal women Most cases occur after age 50
- Obesity Extra fat can increase oestrogen levels
- Polycystic ovary syndrome (PCOS)
- Hormone therapy Especially oestrogen-only therapy without progesterone
- Early menstruation or late menopause
- Never having children
- Tamoxifen use A drug used to treat breast cancer
- Family history Especially Lynch syndrome or colon cancer
Common Symptoms
- Abnormal vaginal bleeding (especially after menopause)
- Heavy or irregular periods
- Pelvic pain or pressure
- Pain during intercourse
- Unusual vaginal discharge
- Unexplained weight loss
Any bleeding after menopause should always be evaluated by a healthcare provider.
How Is It Diagnosed?
- Pelvic examination
- Transvaginal ultrasound: To assess the thickness of the uterine lining
- Endometrial biopsy: A small sample of tissue is taken from the lining of the uterus
- Hysteroscopy: A small camera is inserted to look inside the uterus
- Dilation and curettage (D&C): A surgical procedure to obtain a larger sample
- Imaging (CT, MRI): To check for spread if cancer is confirmed
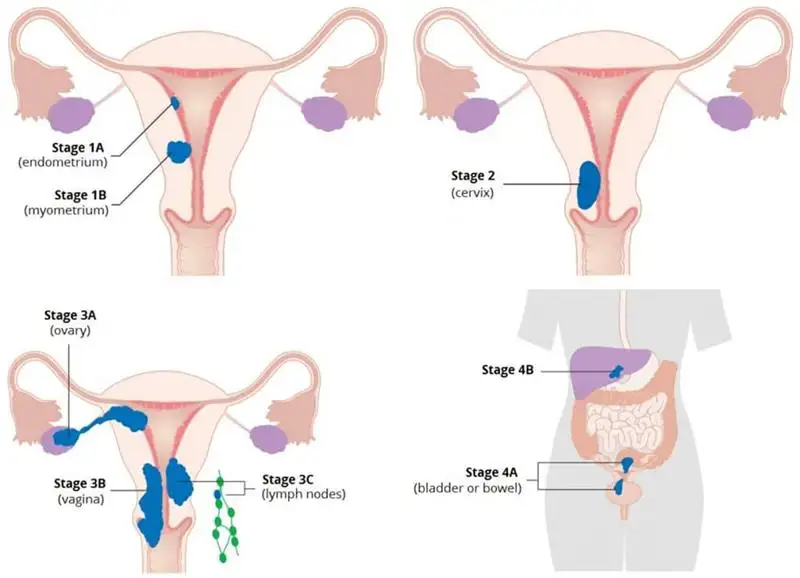
Stages of Uterine Cancer (FIGO)
- Stage I: Confined to the uterus
- Stage II: Spread to the cervix
- Stage III: Spread to nearby structures (e.g., ovaries, vagina, lymph nodes)
- Stage IV: Spread to distant organs (e.g., bladder, bowel, liver, lungs)
Staging guides treatment decisions.
Treatment Options
Treatment depends on the type and stage of cancer, overall health, and whether fertility preservation is desired:
Surgery
- Hysterectomy: Removal of the uterus (often with fallopian tubes and ovaries)
- May include removal of nearby lymph nodes
Radiation Therapy
- Used after surgery in some cases to reduce the risk of loco-regional recurrence
- May also be used if surgery isn’t possible
Hormone Therapy
- Especially for cancers that are sensitive to hormones (e.g., using progestins)
- Sometimes used to preserve fertility in early-stage cases
Chemotherapy
- Used in advanced or aggressive types of uterine cancer
- Can also be used if the cancer returns
Immunotherapy and Targeted Therapy
- Newer treatments that use the immune system or targeted drugs to fight specific types of uterine cancer, particularly those with certain genetic mutations
Living With Uterine Cancer
- Recovery from surgery: Usually takes several weeks
- Menopause symptoms: May occur after surgery if ovaries are removed
- Follow-up care: Essential to monitor for recurrence
- Emotional support: From counsellors, support groups, or survivorship programs is helpful
Prevention and Screening
- There is no standard screening for uterine cancer in average-risk women
- Maintaining a healthy weight , managing conditions like PCOS (Polycystic Ovarian Syndrome), and reporting abnormal bleeding early are important preventive steps
- Women with a family history of Lynch syndrome may need genetic counselling and testing
Recent Advances in Diagnosis and Treatment
1. AI-Driven Diagnostic Tools
Researchers have developed an artificial intelligence model named ECgMPL, which can detect endometrial cancer with 99.26% accuracy by analysing histopathological images. This advancement aims to assist clinicians in early and accurate diagnosis, potentially improving patient outcomes.
2. Immunotherapy Approvals
Dostarlimab: This PD-1 inhibitor has been approved in the UK for patients with advanced or recurrent uterine cancer. Clinical trials have shown that combining dostarlimab with chemotherapy can extend life expectancy and prevent cancer progression in 64% of patients after one year, compared to 24% with chemotherapy alone.
Pembrolizumab: Approved in the US, pembrolizumab has shown efficacy in combination with carboplatin and paclitaxel for treating advanced or recurrent endometrial carcinoma.
3. Targeted Therapy
The combination of pembrolizumab and Lenvatinib has been shown to improve progression-free survival and overall survival in patients with advanced endometrial cancer that is not MSI-H or dMMR and has progressed after other treatments.
FAQs about Uterine Cancer
How long does it take for endometrial cancer to spread?
How long can you live with endometrial cancer?
Survival for endometrial cancer is highly dependent on the cancer's stage at diagnosis, with early detection leading to better outcomes. For instance, the 5-year survival rate is 96% for localized disease but drops to 22% for distant disease, although overall survival rates for all stages combined can reach 84% or higher. Factors like the specific type of endometrial cancer, the patient's overall health, and the chosen treatments also significantly influence how long someone may live.
Is Uterine cancer curable if caught early?
While a diagnosis of uterine cancer can be scary, it is important to know that its most common form—endometrial cancer—is curable, especially if it is caught at an early stage. Uterine cancer is a blanket term for cancers that can develop inside a woman's uterus. The most common treatment for early-stage endometrial cancer is surgery (a hysterectomy), which can cure the cancer. For more advanced cases, or as an additional treatment, radiotherapy or chemotherapy may be used, and immunotherapy can also be an option for certain advanced cases.
How do you prevent endometrial cancer from coming back?
Adopting healthy behaviours such as not smoking, eating well, and staying at a healthy weight might help, but no one knows for sure. Still, we do know that these types of changes can have positive effects on your health that can extend beyond your risk of endometrial cancer or other cancers.
Is endometrial cancer hereditary?
Yes, a small percentage of endometrial cancers (about 2-5%) are hereditary, meaning they are caused by inherited genetic mutations. The most common hereditary cause is Lynch syndrome, an inherited condition that increases the risk of multiple cancers, including endometrial and colorectal cancers. A family history of these cancers can indicate a hereditary link. Other hereditary conditions, such as Cowden syndrome, can also increase the risk of endometrial cancer. A family history of endometrial cancer, especially on the same side of the family, can suggest a genetic link. If you have a strong family history of endometrial cancer or other related cancers, talk to your doctor about genetic counselling and testing. Increased Surveillance: Genetic testing can help identify individuals at high risk, allowing for more proactive screening and management.
What reduces endometrial cancer?
Taking hormonal contraceptives (birth control pills) that combine oestrogen and progestin (combined oral contraceptives) decreases the risk of endometrial cancer.
What drives endometrial cancer?
Changes in the balance of hormones in the body. Examples include obesity, diabetes and irregular ovulation patterns, which might happen in polycystic ovary syndrome. Taking hormone therapy medicine that contains oestrogen but not progestin after menopause increases the risk of endometrial cancer.
Does HRT increase the risk of endometrial cancer?
Yes, unopposed oestrogen-only HRT (Hormone Replacement Therapy) increases the risk of endometrial cancer in women with a uterus because oestrogen stimulates the growth of the uterine lining. However, combined HRT (oestrogen plus progestogen) significantly reduces or eliminates this risk because the progestogen counteracts the effect of oestrogen. Risks depend on the type of HRT, dose, duration of use, and individual factors, so it's crucial to discuss your personal risk profile with a doctor.
Can stress cause endometrial cancer?
Many studies have reported that chronic stress can increase the risk of tumors and promote tumor aggressiveness in various cancers, such as stomach, lung, and skin cancer, yet the relationship between chronic stress and endometrial cancer remains inconclusive, the authors explained.
Where can I find a Specialist for Uterine Cancer?
You can search your Uterine Cancer Specialist on www.ioncosolutions.com