What Is Prostate Cancer?
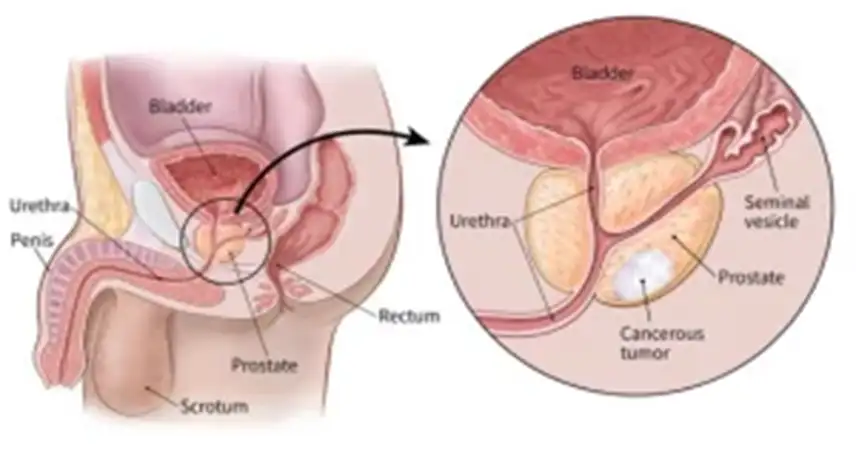
Anatomy of Prostate
The prostate is a small gland about the size of a walnut. It sits under the bladder and in front of the rectum. The prostate is only present in people who are biological males. It is not essential for life, but it is important for reproduction, because it supplies fluids needed for sperm to survive. Sperm are not made in the prostate; they are made in the testes and travel to the prostate through the vas deferens. The seminal vesicles are glands behind the upper end of prostate that store and secrete a large portion of the ejaculate.
The neurovascular bundle is a collection of nerves and blood vessels that run along each side of the prostate, helping to drive erectile function and help with maintenance of urinary control. They travel from the lower spine forward through the pelvis to the penis. Because this bundle sits very close to the prostate, it is often disturbed during prostate cancer treatment and is sometimes directly invaded by more aggressive cancers.
The urethra , a narrow tube that connects to the bladder, runs through the middle of the prostate and along the length of the penis, carrying both urine and semen out of the body.
The rectum is the lower part of the intestines that connects to the anus, and it sits right behind the prostate.
What Is Prostate Cancer?
Prostate cancer is a disease where cells in the prostate gland—a small gland in men that produces seminal fluid—start to grow uncontrollably. It is one of the most common types of cancer in men.
Most prostate cancers grow slowly and may not cause problems for years, but some can be aggressive and spread quickly.
Global Statistics on Prostate Cancer (2024–2025)
Incidence: Prostate cancer is projected to become the most diagnosed cancer in men worldwide. Annual cases are expected to rise from 1.4 million in 2020 to 2.9 million by 2040 , with a significant increase in low- and middle-income countries due to aging populations and improved life expectancy.
Mortality: The number of deaths is anticipated to increase by 85%over the next two decades, from 375,000 in 2020 to nearly 700,000 by 2040 , largely due to late-stage diagnoses in resource-limited settings.
Who Is at Risk?
- Age: Risk increases with age, especially after 50.
- Family history: Having a father or brother with prostate cancer doubles your risk.
- Race: African and Caribbean men are at higher risk.
- Genetics: Inherited mutations (e.g., BRCA1/BRCA2) increases risk.
- Diet & lifestyle: High-fat diets, obesity, and low physical activity may contribute.
Common Symptoms (Often no symptoms in early stages):
- Difficulty starting or stopping urination
- Weak or interrupted urine flow
- Frequent urination, especially at night
- Pain or burning during urination
- Blood in urine or semen
- Erectile dysfunction
- Pain in the back, hips, or pelvis (if cancer has spread)
Always consult a doctor for any persistent symptoms.
How Is It Diagnosed?
- PSA Test: A blood test that measures prostate-specific antigen levels
- Digital Rectal Exam (DRE): A doctor feels the prostate for lumps
- Biopsy: Removal of a tissue sample for lab analysis
- MRI/CT scans or bone scans/PET scans may be used for staging
Staging of Prostate Cancer
- Localized: Confined to the prostate
- Locally advanced: Spread to nearby tissues
- Advanced/metastatic: Spread to lymph nodes or other parts of the body
Staging helps decide the most appropriate treatment plan.
Treatment Options
The treatment options for prostate cancer depend on the patient’s age and general health, PSA level, Gleason score (a grade of how aggressive prostate cancer cells look), and the stage of the cancer and personal preferences.
Localised (confined to the prostate) prostate cancer is treated with either active surveillance, surgery or radiotherapy . Your doctor will select treatment options for you based on a risk stratification scale that is determined by looking at your:
- Gleason score
- PSA level
- Local extent
- Percentage of prostate biopsy cores that are positive for cancer
Metastatic (spread beyond the prostate) prostate cancer is treated with androgen-deprivation therapy (ADT) and/or chemotherapy and novel antiandrogen.
1. Active Surveillance
Who is suitable for Active Surveillance?
Patients with small, low Gleason score prostate cancers which are at low risk of progressing or spreading.
What is Active Surveillance?
Active Surveillance is not a “treatment”. Instead, the physician will monitor the prostate cancer via regular PSA blood tests, digital rectal exams, as well as prostate biopsies.
The goal of surveillance is to avoid treatment-related complications in men who are at low risk of prostate cancer progression. That is because prostate cancer can be slow-growing and might not cause medical problems.
Thus, no medical treatment will be administered unless there is signs or risk of progression of cancer. Curative-intent (Intent to cure) treatment will be delivered if there is clinical progression.
2. Surgery (Prostatectomy)
What is Surgery for prostate cancer?
Radical prostatectomy (removal of the prostate gland) can be performed either via a minimally invasive surgery (robotic or laparoscopic/key-hole) or an open surgery. All prostate tissue is removed during surgery, and the experience of the surgeon is important for the best surgical outcome.
Potential complications of surgery include urinary incontinence and erectile dysfunction.
3. Radiotherapy
What is Radiotherapy for prostate cancer?
Radiotherapy uses radiation to kill cancer cells. There are two types of radiotherapy that can be used in treatment:
-
External beam radiotherapy (EBRT) utilises an external source of radiation to treat the prostate gland and a margin of adjacent normal tissue.
It is for Early-Stage and Locally advanced prostate cancer.
-
Stereotactic Ablative Body Radiotherapy (SABR): For early-stage cancer.

Image from Cancer Research UK
Brachytherapy directly implants a radioactive seed source within the prostate to treat the cancer, thus providing the highest dose of radiation over a very limited distance.
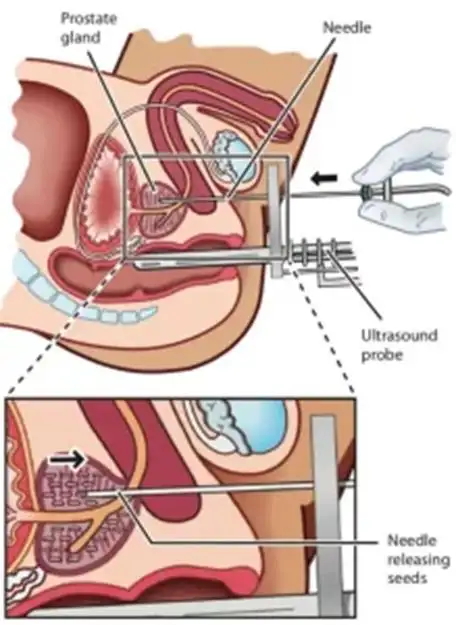
Image from Prostate Cancer Foundation of Aus
Potential Complications
-
Early complications (within a day to a week) include inflammation of rectum, urinary frequency, urgency and dysuria which typically resolves
-
Late complications (after a few months to a year) can include urinary incontinence, erectile dysfunction and narrowing of the urethra.
-
The Treatment of Metastatic Prostate Cancer
Metastatic prostate cancer typically involves the bones. The cornerstone of treatment is androgen-deprivation therapy (ADT), either in the form of surgical castration or medical castration using gonadotrophin-releasing hormone agonist or antagonist. It lowers levels of male hormones (androgens) that fuels cancer growth thus depriving prostate cancer cells of testosterone stimulation, the majority of the cancerous cells will regress. In some situations, novel antiandrogen or chemotherapy may be added to ADT right at the start of treatment, if the patients have metastatic disease at presentation.
If the cancer progresses after ADT, other treatment options include the use of novel antiandrogen, chemotherapy, bone targeting alpha-emitting radioisotope or PSMA radioligand.
There is still ongoing research in terms of:
- Identifying biomarkers for treatment selection to assist doctors in selecting the most appropriate treatment
- Use of active agents in earlier setting, and
- Planning the optimal sequence of treatment types used.
The physician will work closely with the patient to determine the ideal treatment plan that suits the patient’s needs.
Living with Prostate Cancer
- Many men live long, healthy lives with or after prostate cancer
- Discuss side effects like incontinence, erectile dysfunction, or fatigue with your healthcare team
- Consider support groups or counselling
Follow-Up Care
After treatment, regular check-ups and PSA tests are essential to monitor for recurrence or manage side effects.
Recent Breakthroughs in Diagnosis and Treatment
1. AI-Enhanced Imaging for Early Detection
-
Multimodal AI Integration: A study published in January 2025 demonstrated that combining MRI and ultrasound images using AI outperforms traditional methods in detecting clinically significant prostate cancer. This approach achieved higher sensitivity and specificity compared to radiologists, potentially reducing unnecessary biopsies.
-
VERDICT MRI Technique: A new MRI technique called VERDICT (Vascular, Extracellular, and Restricted Diffusion for Cytometry in Tumour) can identify men who do not have prostate cancer, potentially reducing unnecessary biopsies by 90%. This method provides additional information about the prostate's cell structure without the need for new equipment.
2. Advancements in Targeted Therapies
-
Akeega (Niraparib and Abiraterone Acetate): Approved in August 2023, this combination therapy targets BRCA-positive metastatic castration-resistant prostate cancer. It offers a dual-action approach, inhibiting tumour growth and androgen receptor signalling, providing a new treatment option for patients with specific genetic mutations.
-
JANX007 by Janux Therapeutics: In a Phase I trial, this experimental treatment showed unprecedented results, with all 16 participants experiencing at least a 50% decline in PSA levels. The therapy combines T-cell activation with PSMA targeting, offering a promising approach for advanced prostate cancer.
3. Innovative Oral Hormones
-
Relugolix: Approved in 2024, this oral medication provides a convenient alternative to injectable hormone therapies for advanced prostate cancer patients. It eliminates the need for frequent clinic visits and has a favourable side-effect profile, including fewer heart-related risks.
4. Immunotherapy Developments
-
White Button Mushroom Extract: Research from City of Hope suggests that white button mushroom extract may slow prostate cancer progression by inhibiting tumour growth and enhancing immune cells' cancer-fighting abilities. Phase II trial results showed a reduction in myeloid-derived suppressor cells and increased activity of T and natural killer cells in the blood of prostate cancer patients.
Enhanced Radiation Treatment Delivery Technique
Stereotactic Ablative Body Radiotherapy (SABR): Few trials have shown SABR to be non-inferior to conventional radiotherapy in terms of toxicity and survival rates data and is now an established treatment for localised early-stage (low risk and favourable intermediate risk prostate cancer patients. This high-precision radiotherapy treatment drastically reduces the number of sessions required, offering a more convenient and effective option for patients.
MR Linac: SABR treatment delivered on MR Linac machine is further advancement of radiotherapy treatment with daily adaptive radiotherapy planning and treatment as the local anatomy of the prostate and surrounding organs changes daily. Thus, closer treatment margins to the prostate are possible leading to better sparing of the rectum, bladder and bowel with MR Linac machine.
Where can I find a Specialist for Prostate Cancer?
You can search your Prostate Cancer Specialist on www.ioncosolutions.com